
Otitis Media & Ear Tubes
Otitis Media & Ear Tubes
Otitis media, which is an infection or inflammation of the middle ear, affects up to 75 percent of all children before the age of 5 years and accounts for approximately 30 million doctor visits a year in the U.S. Symptoms include ear pain, fever and drainage of fluid from the ear. Although otitis media primarily affects infants and young children, adults can also contract it. Untreated ear infections can lead to more serious complications including hearing loss, perforation of the ear drum, mastoiditis, meningitis and facial nerve paralysis. For effective treatment of otitis media, please contact the experts at ENT of Georgia South.
How Do
We Hear?
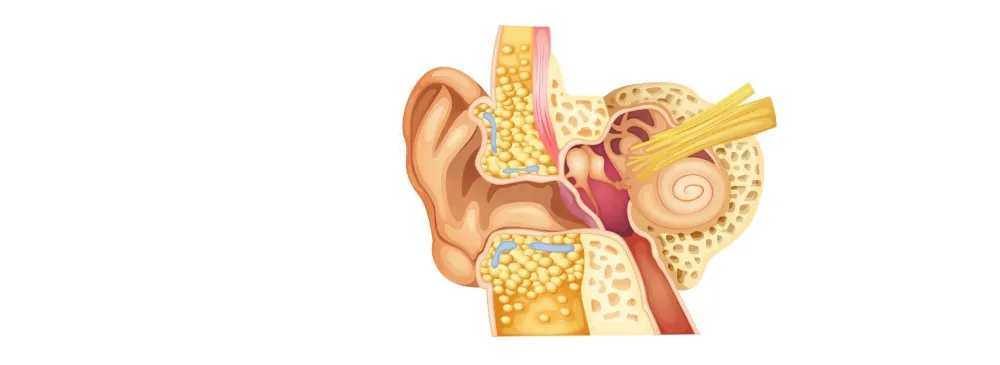
The ear consists of three major parts: the outer ear, the middle ear, and the inner ear. The outer ear includes the pinna--the visible part of the ear--and the ear canal. The outer ear extends to the tympanic membrane or eardrum, which separates the outer ear from the middle ear. The middle ear is an air-filled space that is located behind the eardrum. The middle ear contains three tiny bones - the malleus, incus, and stapes - which transmit sound from the eardrum to the inner ear. The inner ear contains the hearing and balance organs. The cochlea contains the hearing organ with hair cells which convert sound into electrical signals which are associated with the origin of impulses carried by nerves to the brain where their meanings are appreciated.
Why are more children affected by
Otitis Media than Adults?
There are many reasons why children are more likely to suffer from otitis media than adults. First, children have more trouble fighting infections. This is because their immune systems are still developing. Another reason has to do with the child's eustachian tube. The eustachian tube is a small passageway that connects the upper part of the throat to the middle ear. It is shorter and straighter in the child than in the adult. It can contribute to otitis media in several ways.
The eustachian tube is usually closed but opens regularly to ventilate or replenish the air in the middle ear. This tube also equalizes middle ear air pressure in response to air pressure changes in the environment. However, a eustachian tube can be blocked by swelling of its lining or plugged with mucus from a cold or for some other reason, cannot open to ventilate the middle ear. The lack of ventilation may allow fluid from the tissue that lines the middle ear to accumulate. If the eustachian tube remains plugged, the fluid cannot drain and begins to collect in the normally air-filled middle ear.
One more factor that makes children more susceptible to otitis media is that adenoids in children are larger than they are in adults. Adenoids are composed largely of cells (lymphocytes) that help fight infections. They are positioned in the back of the upper part of the throat near the eustachian tubes. Enlarged adenoids can, because of their size, interfere with the eustachian tube opening. In addition, adenoids may themselves become infected, and the infection may spread into the eustachian tubes.
Bacteria reach the middle ear through the lining or the passageway of the eustachian tube and can then produce infection, which causes swelling of the lining of the middle ear, blocking of the eustachian tube, and migration of white cells from the bloodstream to help fight the infection. In this process, the white cells accumulate, often killing bacteria and dying themselves, leading to the formation of pus, a thick yellowish-white fluid in the middle ear. As the fluid increases, the child may have trouble hearing because the eardrum and middle ear bones are unable to move as freely as they should. As the infection worsens, many children also experience severe ear pain. Too much fluid in the ear can put pressure on the eardrum and cause the eardrum to rupture.
What are the Effects of
Otitis Media?
Otitis media not only causes severe pain but may result in serious complications if it is not treated. An untreated infection can travel from the middle ear to the nearby parts of the head, including the brain. Although the hearing loss caused by otitis media is usually temporary, untreated otitis media may lead to permanent hearing impairment. Persistent fluid in the middle ear and chronic otitis media can reduce a child's hearing at a time that is critical for speech and language development. Children who have early hearing impairment from frequent ear infections are likely to experience delay in speech and language development. Only few will experience long term or permanent hearing loss.
How can someone tell if a child has otitis media?
Otitis media is often difficult to detect because most children affected by this disorder do not yet have sufficient speech and language skills to tell someone what is bothering them.
Common Signs to look for:
-
Unusual Irritability
-
Difficulty Sleeping
-
Tugging or pulling at one or both ears
-
Fever
-
Fluid draining from the ear
-
Loss of balance
-
Unresponsiveness to quiet sounds
-
Sitting close to the television
-
Being inattentive

Can anything be done to
Prevent Otitis Media?
Specific prevention strategies applicable to all infants and children such as immunization against viral respiratory infections or specifically against the bacteria that cause otitis media are not currently available. Nevertheless, it is known that children who are cared for in group settings, as well as children who live with adults who smoke cigarettes, have more ear infections. Therefore, a child who is prone to otitis media should avoid contact with sick playmates and environmental tobacco smoke. Infants who nurse from a bottle while lying down also appear to develop otitis media more frequently. Children who have been breast-fed often have fewer episodes of otitis media. Research has shown that cold and allergy medications such as antihistamines and decongestants are not helpful in preventing ear infections. The best hope for avoiding ear infections is the development of vaccines against the bacteria that most often cause otitis media. Scientists are currently developing vaccines that show promise in preventing otitis media. Additional clinical research must be completed to ensure their effectiveness and safety.
How does a child's physician
Diagnose Otitis Media?
The simplest way to detect an active infection in the middle ear is to look in the child's ear with an otoscope, a light instrument that allows the physician to examine the ear canal and the eardrum. Inflammation of the eardrum indicates an infection. There are several ways that a physician checks for middle ear fluid. The use of a special type of otoscope called a pneumatic otoscope allows the physician to blow a puff of air onto the eardrum to test eardrum movement. (An eardrum with fluid behind it does not move as well as an eardrum with air behind it.)
A useful test of middle ear function is called tympanometry. This test requires the insertion of a small soft plug into the opening of the child's ear canal. The plug contains a speaker, a microphone, and a device that is able to change the air pressure in the ear canal, allowing for several measures of the middle ear. The child feels air pressure changes in the ear or hears a few brief tones. While this test provides information on the condition of the middle ear, it does not determine how well the child hears. A physician may suggest a hearing test for a child who has frequent ear infections to determine the extent of hearing loss. The hearing test is usually performed by an audiologist, a person who is specially trained to measure hearing.
How is
Otitis Media Treated?
Many physicians recommend the use of an antibiotic (a drug that kills bacteria) when there is an active middle ear infection. If a child is experiencing pain, the physician may also recommend a pain reliever. Following the physician's instructions is very important. Once started, the antibiotic should be taken until it is finished. Most physicians will have the child return for a followup examination to see if the infection has cleared.
Unfortunately, there are many bacteria that can cause otitis media, and some have become resistant to some antibiotics. This happens when antibiotics are given for coughs, colds, flu, or viral infections where antibiotic treatment is not useful. When bacteria become resistant to antibiotics, those treatments are then less effective against infections. This means that several different antibiotics may have to be tried before an ear infection clears. Antibiotics may also produce unwanted side effects such as nausea, diarrhea, and rashes.
Once the infection clears, fluid may remain in the middle ear for several months. Middle ear fluid that is not infected often disappears after 3 to 6 weeks. Neither antihistamines nor decongestants are recommended as helpful in the treatment of otitis media at any stage in the disease process. Sometimes, physicians will treat the child with an antibiotic to hasten the elimination of the fluid. If the fluid persists for more than 3 months and is associated with a loss of hearing, many physicians suggest the insertion of "tubes" in the affected ears. This operation, called a myringotomy, can usually be done on an outpatient basis by a surgeon, who is usually an otolaryngologist (a physician who specializes in the ears, nose, and throat). While the child is asleep under general anesthesia, the surgeon makes a small opening in the child's eardrum. A small metal or plastic tube is placed into the opening in the eardrum. The tube ventilates the middle ear and helps keep the air pressure in the middle ear equal to the air pressure in the environment. The tube normally stays in the eardrum for 6 to 12 months, after which time it usually comes out spontaneously. If a child has enlarged or infected adenoids, the surgeon may recommend removal of the adenoids at the same time the ear tubes are inserted. Removal of the adenoids has been shown to reduce episodes of otitis media in some children, but not those who are under 4 years of age. Research, however, has shown that removal of a child's tonsils does not reduce occurrences of otitis media. A tonsillectomy and adenoidectomy may be appropriate for reasons other than middle ear fluid.
Hearing should be fully restored once the fluid is removed. Some children may need to have the operation again if the otitis media returns after the tubes come out. While the tubes are in place, water should be kept out of the ears. Many physicians recommend that a child with tubes wear special ear plugs while swimming or bathing so that water does not enter the middle ear.







Our Convenient
Office Locations



Buckhead
1218 W Paces Ferry Rd NW
UNIT 208
Atlanta, GA 30327
Monday - Thursday 8am - 4:30pm
Friday - 8am-2:30pm